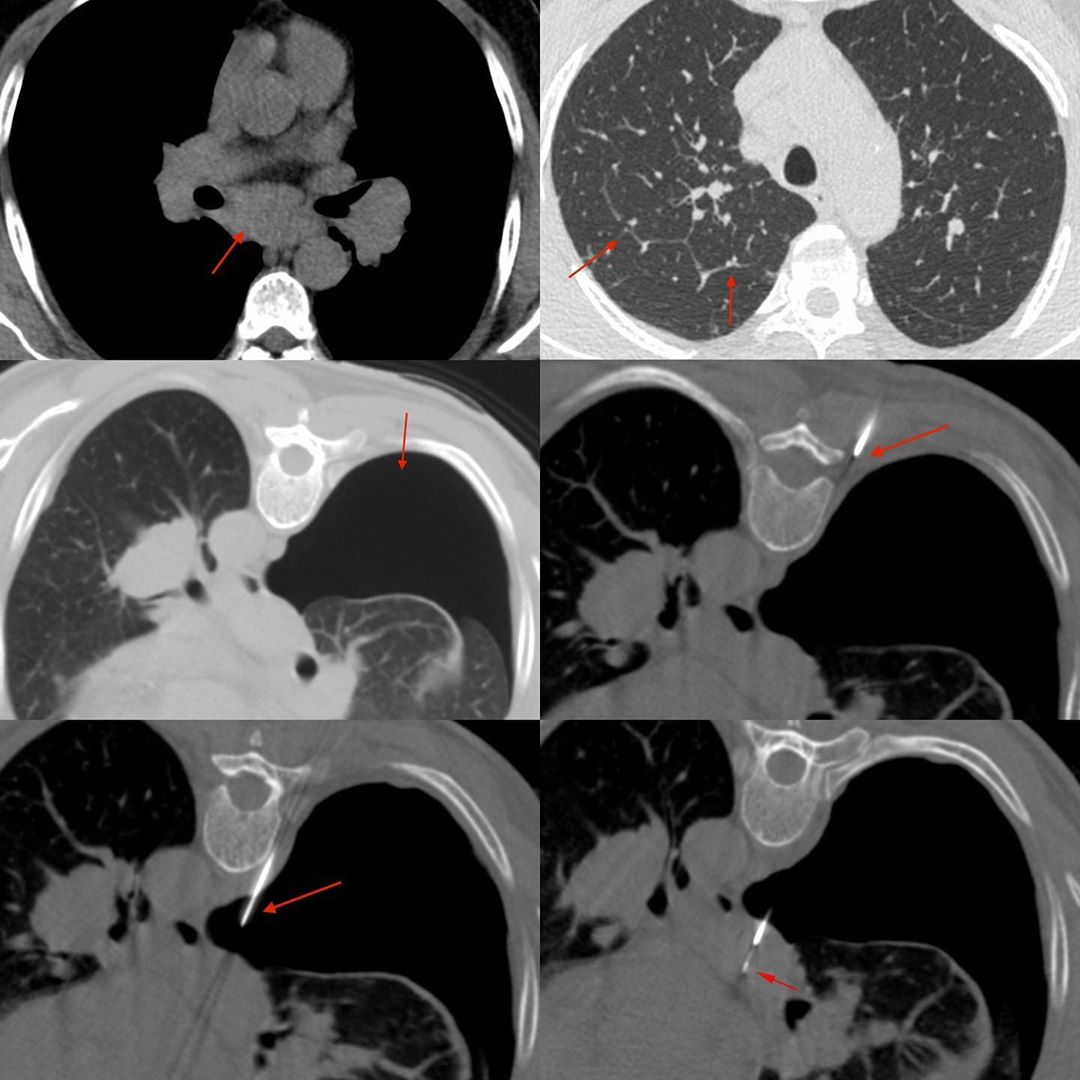
This is a 55 years old man with fever who had subcarinal and bilateral hilar adenopathy with septal thickening in the lungs that suggested sarcoidosis. A subcarinal node biopsy was attempted elsewhere using a trans-pulmonary route, which left him with a pneumothorax.
I started with an extra-pleural approach by injecting saline and lignocaine and creating a space between the pleura and the vertebral body, but eventually had to go through the pneumothorax into the subcarinal node with a 20G coaxial biopsy gun. If you think it through, there is no issue doing that at all.
Yesterday, I showed a case where I went through the loculated pleural collection to biopsy a rib lesion and I thought this is a good companion case to show.
The histopath showed noncaseating granulomatous inflammation of undetermined etiology, which was consistent with the pre-biopsy diagnosis of sarcoidosis.





